- Home
- Patient Care
- Services
- Hip & Knee
- Adult Reconstruction and Hip Preservation Overview
- Hip Impingement
Hip Impingement
Conditions Treated
Femoroacetabular impingement (FAI), also known as hip impingement, as a mechanical or structural disorder of the hip. It can occur in people of all ages, including adolescents and young adults.In the healthy hip, the rounded top of thigh bone (femoral head) “plugs into” the hip socket (acetabular socket) in such a way that the femoral head can move smoothly within the socket. The ball and socket are lined with a thin layer of smooth cartilage that cushions and protects the bones, preventing them from rubbing or grinding against each other. The rim of the hip socket is lined with a special ridge of cartilage called the labrum that further helps to secure the femoral head in place inside the hip socket.
Hip impingement occurs when something prevents the smooth, painless, and free movement of the ball-and-socket joint.
Causes
Hip impingement may be caused by a misshapen femoral head, deformed femoral neck, or a hip socket that covers too much of the femoral head. Over time, repetitive “bumping” or impingement of the femur on the rim of the acetabulum leads to cartilage and labral damage.
People with hip impingement may have been born with a structurally abnormal ball-and-socket joint. In other cases, the hip joint may have become structurally abnormal during development. Repetitive activity involving recurrent movement of the legs beyond the normal range of motion may cause hip impingement, which has been observed in certain athletes (football, baseball, soccer, tennis, hockey, lacrosse players, dancers, and golfers). An injury may also cause symptoms of hip impingement.
Further, certain conditions, such as Perthes disease and slipped capital femoral epiphysis (SCFE), may cause hip impingement.
Types of Hip Impingement
Doctors talk about two main types of hip impingement.
- Cam impingement
- Pincer impingement
Cam impingement occurs because the ball-shaped end of the femur (femoral head) is not perfectly round. This interferes with the femoral head’s ability to move smoothly within the hip socket.
Pincer impingement involves excessive coverage of the femoral head by the acetabulum. With hip flexion motion, the neck of the femur bone “bumps” or impinges on the rim of the deep socket. This results in cartilage and labral damage.
Both conditions can exist at the same time, leading to cam and pincer impingement or combined impingement.
Note that hip impingement can occur with or without the presence of osteoarthritis. In fact, untreated hip impingement is thought to lead to osteoarthritis in many patients.
Symptoms
In the early stages, there may be no symptoms associated with hip impingement or symptoms may be mild or vague. Some typical symptoms include:
- Stiffness in the thigh, hip, or groin
- The inability to flex the hip beyond a right angle
- Pain in the groin area, particularly after the hip has been flexed (such as after running or jumping or even extended periods sitting down)
- Pain in the hip, groin, or lower back that can occur at rest as well as during activity
Diagnosis
An accurate diagnosis of hip impingement is crucial since, left un-treated, hip impingement can lead to cartilage damage and osteoarthritis.
The Joint Preservation, Resurfacing and Replacement department offers comprehensive diagnostic services for hip impingement. Diagnosis begins with a complete medical history and a physical examination. During the physical exam, the range of motion of the hip joint and presence of impingement will be assessed. Other tests may be required, including:
- Radiography (X-rays) which produce two-dimensional images of the hip joint
- Magnetic resonance imaging (MRI) which produces a three-dimensional image including soft tissue cartilage and labrum)
- Computed tomography (CT) scan which takes a series of small images at different angles and then applies a computer algorithm to construct a three-dimensional image of the hip. A CT scan is often used to show doctors the detailed structure of joints.
Treatment
The Joint Preservation, Resurfacing and Replacement department will discuss appropriate treatment options with you. Some patients are able to successfully manage hip impingement with conservative therapies, including:
- Reducing certain types of physical activity
- Physiotherapy
- >Pain management
- Injections
In some cases, surgical intervention is recommended. Such surgery may be minimally invasive (arthroscopic) or open. Arthroscopic treatment is the more common and can correct most impingement deformities. Severe or complicated impingement deformities are best managed as open surgery in order to insure full correction of the deformity. In some cases, an osteotomy (literally “bone cutting”) procedure can be performed in such a way that it relieves the impingement of the hip joint. By realigning the joint properly, the abnormal contact can be reduced or eliminated. An abnormally shaped femoral head or hip socket can often be reshaped with osteoplasty or debridement. In such cases, the surgeon can “clean” or “sculpt” the ball-and-socket joint for a smoother fit.
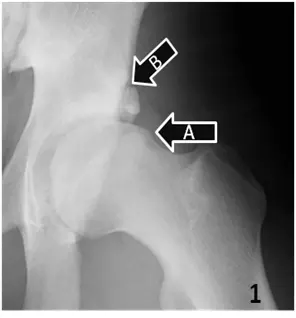
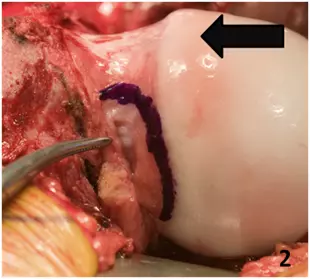
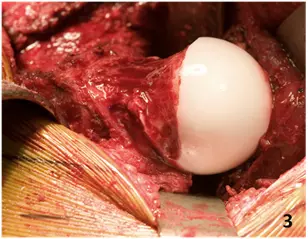

A lateral radiograph of the hip in a 17-year-old male with hip pain is shown (1). The prominence of the femoral head-neck junction is demarcated with arrow A. This is consistent with cam impingement. This patient also has a fracture of the acetabular rim as demarcated by arrow B. At surgery (2) the femoral head demonstrates the damaged articular cartilage (arrow) and prominence of the femoral head. The surgical correction of this deformity (3) and the post-operative x-ray (4) are shown. This patient had an excellent clinical result after treatment of this impingement deformity.
For young, athletic individuals, arthroscopic or open repair of the joint may be appropriate. Arthroscopy is a specialized, minimally invasive procedure to repair the joint. Open surgery is indicated for more severe cases. Both arthroscopic and open procedures can provide excellent clinical results. After surgical repair, the patient typically undergoes a period of physical rehabilitation that can last three to four months.
In some cases, people with hip impingement may need to have a total hip replacement.
The choice of treatment depends in part on your condition, amount of arthritis in the joint, your age and activity level, and your preferences. We will help you understand the risks and benefits of various treatment options.
Facts and Figures
- The rate at which hip impingement occurs in the general population is not known
- Hip impingement commonly affects active adolescents and young adults
- Untreated hip impingement may lead to hip osteoarthritis
- Surgical management of hip impingement is successful in approximately 80% of patients at short-term follow-up.